Free Hipaa Medical Release Authorization Form Pdf
“1-800-medicare authorization to disclose personal health information” form by law, medicare must have your written permission (an “authorization”) to use or give out your personal medical information for any purpose that isn't set out in the privacy notice contained in the medicare & you handbook. The medical record information release (hipaa), also known as the ‘health insurance portability and accountability act’, is included in each person’s medical file. this document allows a patient pdf to authorization form release information hipaa medical to list the names of family members, friends, clergy, health care providers, or other third (3rd) parties to whom they wish to have made their medical information available. I, or my authorized representative, request that health information regarding my care and treatment be released as set forth on this form. i understand that: 1. Of the hipaa-compliant authorization form to release health information needed for litigation this form is the product of a collaborative process between the new york state office of court administration, representatives of the medical provider community in new york, and the bench and bar, designed to produce a standard official form that.
Hipaa Authorization For Research
Fill hippa form, edit online. fill hipaa consent form pdf: try risk free by everyone who wants to share the medical information with someone else now it authorization for release of protected health information, dhcs 6247, eng. The hipaa release form must be completed and signed before a health care provider can release an individual’s healthcare information. the health insurance portability and accountability act was created in 1996 with the sole purpose of protecting the personal information of each citizen’s medical information.
Hipaa Release Form Hipaa Journal
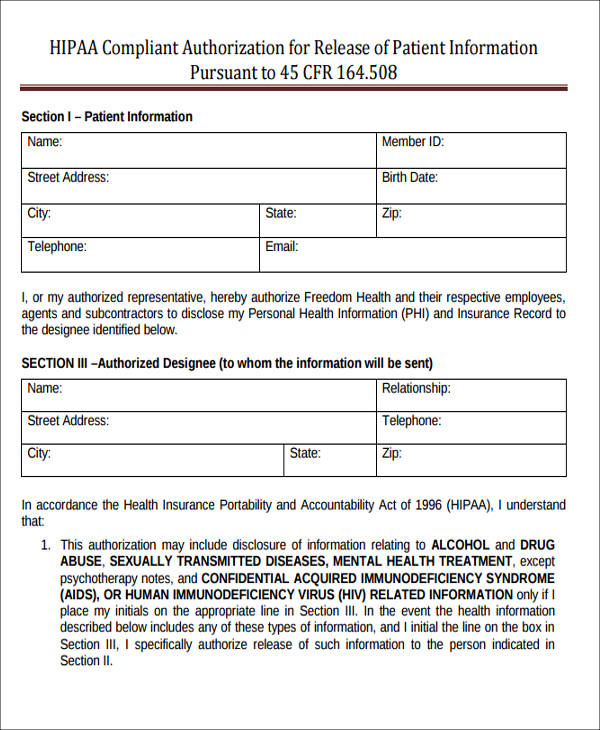
Hipaa compliant authorization for the release of patient telephone messages, and records received by other medical providers. all physical, occupational and rehab requests, consultations and progress notes. hipaa compliant authorization form for the release of patient information pursuant to 45 cfr 164. 508. Sample authorization language for research uses and disclosures of individually identifiable health information by a covered health care provider authorization to use or disclose (release) health information that identifies you for a research study optional elements:. Sample authorization language for pdf to authorization form release information hipaa medical research uses and disclosures of individually identifiable health information by a covered health care provider. authorization to use or disclose (release) health information that identifies you for a research study. Section i veteran's identification information general release for medical provider information to the department of veterans affairs (va) instructions complete and attach this form with a signed va form 21-4142, authorization to disclose information to the department of veterans affairs (va). if you.
Page 1 of 3 hipaa release form please complete all sections of this hipaa release form. if any sections are left blank, this form will be invalid and it will not be possible for your health information to be shared as requested. Authorization for release of medical records to request release of medical information please complete and sign this form i, _____hereby voluntarily authorize the disclosure of information from my health record. (name of patient) patient information:. If you want your healthcare provider to send your medical records, this form must be signed and dated by the patient or the patient’s legal representative. new york state department of health state disability review unit instructions for completing the authorization for release of health information pursuant to hipaa doh-5173 (4/16) page 2 of 2. Nov 25, 2020 · this law was primarily passed due to proliferation of data breaches concerning health information. this hipaa release form pdf template is a standard release authorization form for disclosure of health information for healthcare and health insurance providers which the subject or person consents on disclosing his health information to a certain.
Hipaa authorization to release patient information i hereby request that privia medical group use / disclose my protected health information i understand that i have the right to receive a copy of my phi in the form and format&nb. A hipaa release of information form is also a means of preventing anyone from using your medical information in any other way than what was originally intended. parent information forms share a somewhat similar function to a hipaa release of information form in the sense that it is a means of limiting information only to authorized individuals. Claimant's authorization to disclose health information (pursuant to hipaa) instructions to the claimant: the health insurance portability and accountability act of 1996 (hipaa) set standards for guaranteeing the privacy of individually identifiable health information and the confidentiality of patient medical records.
Feb 09, 2021 · what must be included on a hipaa authorization form? a hipaa authorization is a detailed document in which specific uses and disclosures of protected health are explained in full. by signing the authorization, an individual is giving consent to have their health information used or disclosed for the reasons stated on the authorization. Medical treatment ❑ medical condition verification ❑ disability ❑ fmla ❑ workers' comp. kaiser permanente may release this information to: ❑ check if same as above unit listed for your region of service on the reverse side of this. Purpose of disclosure. □at the patient's request. description of information to be released: □ pertinent summary (includes all * items). □ admission form.
Authorization for release of medical record information. patient name: please note: copy fee may be charged for medical records. dates and type of not sign this form in order to assure treatment. i understand that i . See 45 cfr 164. 508(a)(3). a communication does not require an authorization, even if it is marketing, if it is in the form of a face-to-face communication made by a covered entity to an individual; or a promotional gift of nominal value provided by the covered entity. for example, no prior authorization is necessary when:. 4. this medical information may be used by the person i authorize to receive this information for medical treatment or consultation, billing or claims payment, or other purposes as i may direct. 5. this authorization shall be in force and effect until _____ (date or.
To this authorization may not further use or disclose the medical information unless another authorization is obtained from me or unless such disclosure is . Authorization to disclose protected health information. developed for form that complies with hipaa, the texas medical privacy act, and on a failure to sign this authorization form, and a refusal to sign this form will not . Educational records that may contain health information. as indicated on the form, specific authorization is required for the release of information about certain sensitive conditions, including: • mental health records pdf to authorization form release information hipaa medical (excluding “psychotherapy notes” as defined in hipaa at 45 cfr 164. 501). • drug, alcohol, or substance abuse records.
Aug 10, 2020 · but before sharing phi with researchers, your patient will need to sign a hipaa medical records release form. 4. when the patient’s release form has expired. normally, release forms fulfill one-time needs, such as releasing information to a family member in connection with a specific procedure. A. i have a right to revoke this authorization in writing at any time, except to the extent information has been released in reliance upon this authorization. b. the information released in response to this authorization may be re-disclosed to other parties. c. my treatment or payment for my treatment cannot be conditioned on the signing of this.
